UPDATED: new contract analysis
P3 Pharmacy,
01 Aug 2019![]() 3 Min
3 Min
P3 Pharmacy,
01 Aug 2019![]() 3 Min
3 Min
P3 Pharmacy,
01 Aug 2019![]() 3 Min
3 Min
On one page: the headline and immediate analysis of the five year agreement announced by the Pharmaceutical Services Negotiating Committee.
First thoughts from P3pharmacy's editors
Representative comment from NPA, CCA, RPS, McKesson UK, Phoenix UK
Front line opinion from Dorset contract Mike Hewitson
Our anonymous community pharmacist takes a positive view of the last chance saloon
More detail needed but the numbers show where to invest, says RWA's Paul Counter
At a time when community pharmacy is facing increasingly difficult times, the funding package is of crucial importance to contractors.
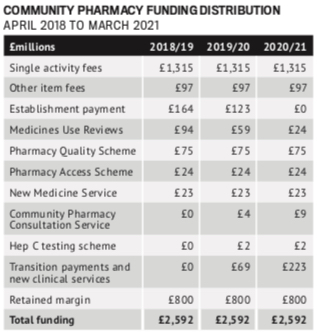 Total funding is £2.592 billion per annum for five years from 2019/20 to 2023/24. This is also the same total as 2018/19.
Total funding is £2.592 billion per annum for five years from 2019/20 to 2023/24. This is also the same total as 2018/19.
P3PHARMACY COMMENT
While a 5-year static funding deal may provide certainty, it creates neither the obvious resources nor the necessary enthusiasm required for transformative change.
The loss of the automatic establishment payment means that while the funding is retained, contractors will need to do more to earn it back. It does however, remove one line or argument from anti-pharmacy hawks, that pharmacies are paid “just for being there”.
The Pharmacy Quality Scheme (PQS) – the new name for the Quality Payments Scheme from October 2019 – will be worth £75m in each of the next five years.
It will help to underpin a contract which focuses on services. An ongoing programme of activity will ensure that community pharmacies deliver health benefits to patients.
New requirements (in addition to the current ones, which will become Terms of Service requirements from April 2020) are:
P3PHARMACY COMMENT
The PQS is critical to ensure the safety, quality and consistency of clinical services. The elements of the new PQS reflect wider NHS and societal priorities, making community pharmacy a part of mainstream delivery. They also reflect a mainstreaming of models which have been tested in the past – the Community Pharmacy Safety Group has conducted valproate and lithium audits, for example. Sepsis awareness has been promoted by multiples and the NPA, as well as by P3pharmacy and our sister titles.
Announced as a contract that is more focused on patient care services, a raft of them are planned over the next five years:
MURs to be phased out
Community Pharmacist Consultation Service (CPCS) – NHS 111 and GP referrals
Medicines reconciliation service
Other activities
Future services
P3PHARMACY COMMENT
The loss of MURs has been widely trailed. They never evolved from 2015, and anecdotally they are of variable quality, which is almost the same point. With clinical pharmacists in general practice and PCNs going to be delivering structured medication reviews, they were surplus to requirements. At least the funding is being recycled into different services, but the lesson from the MUR experience is that delivery, quality and patient outcome are important. It may be that pharmacy needs to look again at the New Medicines Service, which has a very clear evidence base, to ensure that any additional therapeutic areas added in are joining a service that is subject to a continuous improvement cycle.
PSNC has agreed to have discussions with DHSC and NHSE&I on how best to commission IT in community pharmacy and to explore ways to make dispensing more efficient, to free up pharmacist and pharmacy team time and capacity.
Topics to be covered include:
P3PHARMACY COMMENT
There’s a lot of work in here but there are probably some potential upsides in an otherwise flat funding package that will be eaten away by inflation and the inevitable cost pressures that will accrue over five years in most service businesses. There’s some long-standing irritants, like part pack dispensing, that might finally achieve some resolution – OPD was due to be implemented as long ago as 1992 – but there’s lots of detailed work needed. Five years might not be enough.
First thoughts from P3pharmacy's editors
Representative comment from NPA, CCA, RPS, McKesson UK, Phoenix UK